
University of New South Wales Law Journal

|
|
Home
| Databases
| WorldLII
| Search
| Feedback
University of New South Wales Law Journal |
|
CLAIMANT LAWYER USE IN ROAD TRAFFIC INJURY COMPENSATION CLAIMS
1
2
CLARE E SCOLLAY[*], JANNEKE BERECKI-GISOLF[**], BECKY BATAGOL[***] AND GENEVIEVE M GRANT[****]
In injury compensation schemes, claimants engage lawyers to navigate the claiming process, access benefits, and resolve disputes. As a result, lawyers can play a central role in facilitating claimant access to entitlements, and shaping claimant experiences and outcomes. This article presents findings from the largest empirical investigation of lawyer use in a single compensation scheme: using evidence from almost 50,000 claims in the road traffic injury scheme in Victoria, Australia, the socio-demographic, crash, injury, and recovery factors associated with lawyer use are identified, and explanations for these relationships explored. The analysis shows that some claimants who struggle to access lawyers in other contexts are supported to do so in this scheme. The findings highlight opportunities for improving access to justice within and outside compensation settings.
Road traffic crashes cause an estimated 50 million injuries each year[1] and account for much of the global burden of disability.[2] The magnitude of this problem continues to grow as the quality of healthcare improves and the number of individuals surviving their injuries increases.[3] As a result, road traffic injuries have been designated a public health priority in Canada,[4] the United States,[5] the European Union,[6] parts of Asia[7] and Africa,[8] Australia,[9] and New Zealand.[10] Although the policy focus is on reducing the number of serious road traffic injuries, there is also a growing emphasis on improving recovery outcomes.
Crash survivors often engage with a range of services in recovering from road traffic injuries, including health, legal, and financial services.[11] In many jurisdictions, statutory injury compensation schemes facilitate access to these and other benefits, with the objective of returning injured persons to health and work as efficiently and effectively as possible.[12] There are considerable inconsistencies in the nature and extent of the benefits provided by these schemes. In Australia, for example, all states and territories provide long-term care and support to persons who sustain significant and permanent injuries, irrespective of fault;[13] however, for other injured persons, there is substantial variation in the benefits available, and the basis on which these benefits are provided.[14]
In compensation schemes, injured persons may engage lawyers for help with navigating the claiming process, accessing benefits, and resolving disputes.[15] Legal services can play an important role in enabling claimants to access their legal entitlements, particularly when they might struggle to do so otherwise, whether because of their own disadvantage or complexities in scheme design. As a result, lawyer use is often associated with access to justice, which has been described as the extent to which claimants can enforce their rights through fair and open processes.[16] Some studies suggest that claimant lawyer use is also associated with negative recovery outcomes, including physical and mental ill-health;[17] longer treatment times;[18] delays in, and lack of, claim closure;[19] and lower perceived fairness of compensation processes.[20] These associations are attributed to extended legal proceedings that prolong claimant exposure to compensation schemes;[21] the adversarial nature of the claiming process;[22] and implicit or explicit encouragement of claimants to remain symptomatic to maximise their likelihood of succeeding in their claims.[23]
Importantly, however, these studies have been unable to determine whether the relationship between lawyer use and negative recovery outcomes is causal in nature, so it is unclear whether lawyer use leads to poor recovery, or poor recovery leads to lawyer use.[24] Claimants experiencing slower recoveries may be more likely to consult a lawyer than those who recover faster.[25] In addition, lawyers perform a gatekeeping function, filtering out claims that they are reluctant to pursue.[26] This is because legal services in the personal injury sector are often provided under conditional or ‘no win, no fee’ agreements,[27] in which some or all legal costs are dependent on the successful outcome of the matter.[28] For a lawyer to act under this type of agreement, they must conclude that the legal fees paid out of the damages will be sufficient to cover their costs and turn a profit.[29] As a result, lawyers favour cases where there is a strong likelihood of succeeding in the claim and achieving substantial damages.[30] In personal injury cases, these factors depend on the severity and (in Australia) permanence of claimant injuries. As a result, injury severity and expected permanence play a critical role in case selection by lawyers, and in turn legal service use by claimants.[31]
Notably, there has been little research into the relationship between injury severity, lawyer use, and recovery outcomes, and the few existing studies have yielded inconsistent results. Gun and colleagues identified a strong association between initial pain index and lawyer use,[32] and between lawyer use and negative recovery outcomes (including lack of improvement in pain outcome score, longer treatment time, delayed claim closure, and delayed return to work).[33] The association between lawyer use and these outcomes (except delayed return to work) remained after adjusting for initial pain index (although pain is not necessarily indicative of injury severity).[34] Conversely, Casey and colleagues found that the clinical whiplash grading of claimants who retained a lawyer did not differ from that of claimants who did not, although the former group presented with a worse health profile and greater work disability at one year post-injury.[35] These authors posit that some claimants have a specific health profile that ties them to the compensation scheme for a long period of time, resulting in both negative recovery outcomes and lawyer use.[36] This profile is not necessarily linked to injury severity, but may be evidenced by poor fitness, a low pain tolerance, a tendency to catastrophise, and the development of anxiety, depression, and other complications.[37]
Studies conducted in compensation settings suggest that lawyer use is also associated with individual-level factors beyond injury severity, including higher initial disability and work disability, lower baseline mental health and household income, and speaking a language other than English in the home.[38] However, the samples used in these studies are limited to injured persons with whiplash[39] or orthopaedic diagnoses[40] in the New South Wales (‘NSW’) road traffic injury compensation scheme, at a time when it was primarily fault-based. Accordingly, the applicability of the findings to claimants with a broader range of injuries and in other compensation schemes is unclear. This is particularly so given that claimant decisions about engaging legal services are influenced by compensation scheme design,[41] and experiences and exposures of claimants in one scheme are not necessarily equivalent to those of claimants in other schemes.[42]
Overall, the factors associated with lawyer engagement in compensation schemes are not well understood. In particular, the extent to which injury severity and recovery contribute to decisions to use legal services remains unclear. Empirical analysis of these relationships is required to improve our understanding of the operation of injury compensation schemes as the law’s primary response to the legal problem of injury, as well as the justice that claimants experience. The aims of this study are, therefore, to (a) determine the amount of lawyer use that is explained by injury severity, (b) identify additional individual-level socio-demographic, crash, and injury factors associated with lawyer use, and (c) determine the extent to which lawyer use is explained by short- and long-term recovery outcomes, in the road traffic injury compensation scheme in Victoria. This approach enables us to identify the individual-level factors associated with lawyer use among compensation claimants with a broad range of injuries and in a blended scheme (ie, a scheme that includes both no-fault and fault-based benefits). Additionally, it allows us to clarify the roles played by injury severity and recovery factors in contributing to lawyer engagement.
In Victoria, persons injured in transport crashes involving a car, motorcycle, bus, train, or tram are eligible to claim compensation through the State insurer, the Transport Accident Commission (‘TAC’).[43] The TAC is funded through annual car registration payments made by Victorian motorists, as well as income generated from investments. The TAC operates as a single-insurer Compulsory Third Party (‘CTP’) scheme that provides a blend of no-fault and common law benefits. In this scheme, injured persons are eligible for income replacement, medical, rehabilitation, and lifetime care costs irrespective of fault.[44] If a claimant has a permanent whole-person impairment assessed as being above 10%, they may also be entitled to a no-fault impairment lump sum payment.[45] Claimants are eligible for common law damages for pain and suffering and pecuniary loss if another party was negligent in their crash circumstances, and their injuries exceed a minimum threshold based on either their permanent whole-person impairment or a narrative test of the ways in which their injuries have affected their capacity to engage in valued activities.[46] Permanent impairment and common law damage claims must typically be made within six years of the crash.[47]
Where a legally represented claimant makes a successful claim for an impairment lump sum benefit or common law damages,[48] or a dispute about a no-fault benefit is resolved in the claimant’s favour, the TAC will make a contribution to the claimant’s legal costs.[49] Where a claim is litigated in a tribunal or court, legal costs will follow the event such that the successful party will typically be entitled to an order for costs against the unsuccessful party. The precise amount and proportion of costs covered depends on the application of provisions contained in the TAC Protocols (a series of agreements made between signatory plaintiff law firms, the TAC, and the Law Institute of Victoria),[50] as well as orders made by the relevant tribunal or court. This proportion often falls short of full coverage, meaning that claimants will most often fund some part of the costs themselves once their claim is resolved, out of compensation they receive. There are also circumstances in which the TAC may recover costs from unsuccessful claimants. For example, in some matters, if the TAC makes a settlement offer that the claimant rejects, and the order subsequently made by a tribunal or court is not more favourable than that offer, the TAC may seek an order that the claimant pay the legal costs incurred by the TAC after the offer was made.[51]
Personal injury lawyers acting for TAC claimants almost exclusively operate on a ‘no win, no fee’ (or conditional costs) basis, meaning that a claimant will only be charged for the lawyer’s professional fees in the event that they achieve a successful outcome. Legal costs regulation in Victoria permits lawyers operating on a conditional basis to charge a ‘success fee’ in the form of an uplift of up to 25% of the legal costs (excluding disbursements) that would otherwise be payable.[52] Contingency fees, where a lawyer agrees with a client that they will charge a percentage of compensation recovered by the client, are prohibited.[53]
II MATERIALS AND METHODS[54]
To investigate lawyer use by claimants, we established a unique dataset based on compensation claim data. At the time of this study, administrative data relating to claims lodged with the TAC were housed in the deidentified Compensation Research Database (‘CRD’) at Monash University.[55] Data for claims relating to crashes that occurred between 1 January 2007 and 31 December 2009 were extracted for use in this study (N=53,471 claims made by N=52,937 claimants). Claims for crashes that occurred interstate[56] and for fatalities[57] were removed from the data (N=3,378 claims made by N=3,335 claimants). Finally, in cases where there were multiple claims per claimant within the study period, only the first claim was included, resulting in the removal of a further 491 claims.[58]
The final sample (N=49,602 claims and claimants) included more males (52.4%) than females (47.6%) and the greatest proportion of claimants were in the 15 to 24 year age category (22.7%). Most claimants lived in a major city (73.4%)[59] and approximately half were within the top five socio-economic status (‘SES’) deciles (52.7%). Few claimants had made a prior claim in the seven years preceding their crash date (1.4%) or used the services of an interpreter or translator (0.8%). Most claimants were injured in a crash that involved more than one vehicle (60.0%) and less than half were driving at the time of the collision (46.9%). The greatest proportion of claimants were not hospitalised following the crash (62.1%) and sustained whiplash injuries (31.3%). Relatively few claimants reported ongoing work disability, mental health, or pain issues at 3 months (19.9%, 17.8%, and 14.4%, respectively) or 12 months (17.4%, 17.0%, and 14.1%, respectively) post-crash.[60]
To maximise the capture of lawyer use in this study, six years of follow-up claim data were obtained for all claims. This follow-up period was selected as claims for impairment lump sum and common law payments, both of which involve a high proportion of lawyer use,[61] must typically be made within six years of the crash date.[62] However, as claimants can engage lawyers for other purposes at any time during their claims, this follow-up period is unlikely to capture all lawyer use. Prior research in the same jurisdiction has shown that a four-year follow-up period captures 85% of lawyer use.[63]
Socio-demographic, crash, injury, recovery, and lawyer use data were extracted for use in descriptive and logistic regression analyses.
Socio-demographic variables included age, gender, interpreter use (as a proxy for a primary language other than English), prior claiming, remoteness (primary Accessibility and Remoteness Index (‘ARIA+’) grouping),[64] and SES (Index of Relative Socio-economic Advantage and Disadvantage (‘IRSAD’) State Decile).[65] Interpreter use was defined as the presence of a payment for interpretation or translation services, or to an interpretation or translation service provider, within the follow-up period; this is likely to underestimate the number of claimants who required such services, as some claimants may have enlisted family members or friends to provide these on an informal and unpaid basis, or been unaware that these services were available and thus foregone them. Prior claiming was defined as the presence of an additional TAC claim made by the same claimant in the seven years preceding the crash.
Crash variables included number of vehicles involved in the crash and claimant road user group.
Injury variables included injury type, length of hospital stay, and injury severity. Injury type was defined based on standard categories in the CRD. Length of hospital stay was calculated based on the number of full days for which the claimant was an inpatient; emergency department (‘ED’) presentations and outpatient attendances were excluded from this count. ICD-based Injury Severity Scores (‘ICISSs’) were calculated by mapping the International Statistical Classification of Diseases, Tenth Revision, Australian Modification, (‘ICD-10-AM’) codes provided by the TAC to the Survival Risk Ratios (‘SRRs’) created for Australia;[66] these codes were only available for claimants who had been hospitalised. The SRRs were then multiplied to create an overall ICISS; multiplication was used to ensure maximal use of available data.[67] ICISSs were separated into quartiles for use in the analyses, and were reverse-scored so that the lowest quartile contained the least severe (or most survivable) injuries, whilst the highest quartile contained the most severe (or least survivable) injuries.
Short- and long-term recovery outcomes were assessed at 3 and 12 months post-crash respectively, and included work disability, mental health, and pain indicators. These outcomes were identified using a combination of TAC benefit codes, Medicare Benefit Schedule codes, and Pharmaceutical Benefit Schedule (‘PBS’) codes from the payment data. For the PBS codes, information on the PBS website was used to identify the generic name, form, strength, and pack size of each medication.[68] These were then matched to Anatomic Therapeutic Chemical (‘ATC’) classification codes using information on the ATC website.[69] Medications with ATC codes starting with ‘N02’ were identified as analgesics, ‘N02A’ as opioid analgesics, ‘N05A’ as antipsychotics, ‘N05B’ as anxiolytics, and ‘N06A’ as antidepressants.[70]
Work disability was defined as the presence of fortnightly payments for loss of earnings or loss of earning capacity within the relevant time period. For example, work disability at three months was defined as the presence of fortnightly payments for loss of earnings or loss of earning capacity that commenced before or at three months post-crash and concluded at or after three months post-crash. Mental health indicators were defined as the presence of payments for (a) psychological services, (b) psychiatric services, (c) GP visits that addressed mental health issues, or (d) antidepressants, antipsychotics, or anxiolytics, within the relevant time period. Pain indicators were defined as payments for analgesics or opioid analgesics within the relevant time period. As there was substantial overlap between the recovery indicators, in the regression analyses these indicators were combined into a measure of the number of adverse recovery outcomes experienced.
Lawyer use within six years post-crash was identified through the presence of a solicitor engagement date or payment for legal services in the six-year follow-up period. The solicitor engagement date was calculated by the TAC as the earliest of the following dates: (a) solicitor start date entered into the system by TAC staff, (b) dates derived from legal documents, or (c) dates derived from references to solicitors in claim notes.
To compare the socio-demographic, crash, injury, and recovery profiles of claimants who did and did not engage legal services within the six-year follow-up period, descriptive analyses were used. To assess whether observed differences were statistically significant, chi-square tests were used (as all variables were categorical).
To determine associations between socio-demographic, crash, injury, and recovery indicators and lawyer use within six years post-crash, logistic regression analyses were used. Claimants with injuries that were catastrophic, or sustained aboard a train or tram, were excluded from these analyses due to small cell counts. Interpreter use was excluded as an input into these analyses for the same reason.
As injury severity data were only available for claimants who had been hospitalised, the dataset was split into hospitalised and non-hospitalised cohorts. For the hospitalised cohort, to assess the unadjusted influence of injury severity on lawyer use, this variable was entered into a logistic regression alone. Next, to identify additional individual-level factors associated with lawyer use, the socio-demographic, crash, and injury variables were entered into a logistic regression (‘Model One’). Injury severity was then added to this model (‘Model Two’). Finally, to determine the influence of short- and long-term recovery outcomes on lawyer use, recovery variables at 3 (‘Model Three’) and 12 (‘Model Four) months were added. Finally, Models One, Three, and Four were replicated in the non-hospitalised cohort.
The Link Test[72] and Akaike Information Criterion (‘AIC’)[73] were used to indicate goodness-of-fit and compare model performance, respectively. The Tjur ‘R2’ test was used to indicate the amount of variation in lawyer use explained by each model.[74]
Overall, 15.5% of claimants used lawyers within the six-year follow-up period; this proportion was higher among hospitalised (24.9%) than non-hospitalised (10.0%) claimants. Most claimants who used lawyers had common law claims (50.2%), followed by no-fault claims without impairment lump sum components (39.8%), and no-fault claims with impairment lump sum components (10.0%). For the socio-demographic variables, bivariate tests revealed statistically significant differences in the distributions of age, gender, interpreter use, prior claiming, remoteness, and SES between claimants who did and did not engage lawyers (see Table 1). Specifically, claimants who engaged lawyers were more likely to be aged between 35 and 74 years; be male; have used an interpreter; have a prior claim; live in outer regional, remote, or very remote Victoria; and be in the lowest six SES deciles relative to claimants who did not. Notably, there was a statistically significant negative linear relationship between SES and the proportion of claimants who used legal services (R2=0.91, F(1,8)=89.94, p<0.0001; this correlation was computed based on aggregate data): that is, as SES increased, lawyer use decreased (see Figure 1).
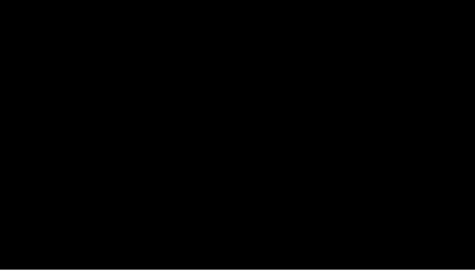
Figure 1: Proportion of Claims That Did and Did Not Involve Lawyer Use by SES Decile
For the crash variables, there were significant differences in the distributions of number of vehicles involved in the crash and claimant road user group between those who did and did not use lawyers (see Table 1). Specifically, claimants who used a lawyer were more likely to have been involved a single-vehicle crash, and less likely to have been involved in a multi-vehicle crash, than those who did not. The most notable differences for claimant road user group were that those who used a lawyer were more likely to be pedestrians, and less likely to be drivers, relative to those who did not. For the injury variables, there were significant differences in the distributions of injury type and length of hospital stay between claimants who did and did not use lawyers. The most notable differences for injury type were that claimants who used lawyers were more likely to have ‘orthopaedic’ (limb fracture) injuries, and less likely to have ‘musculoskeletal’ (whiplash) or ‘other’ (abrasion, contusion, and laceration) injuries, than those who did not. Claimants who used lawyers were also more likely to have spent more than seven days in hospital, and less likely to have spent no days in hospital, compared to those who did not. Finally, for the recovery variables, there were significant differences in the distributions of work disability, mental health, and pain indicators between those who did and did not engage lawyers. Specifically, claimants who engaged lawyers were more likely to have work disability, mental health, and pain indicators (‘negative recovery outcomes’) at 3 and 12 months post-crash relative to those who did not.
Table 1: Characteristics of Compensation Claimants with and without Lawyer Use
|
All Claims
|
Claims with No Lawyer Use
|
Claims with Lawyer Use
|
Chi-Square
|
|||||
|
|
N
|
N
|
Column %
|
Row %
|
N
|
Column %
|
Row %
|
χ2
|
|
N
|
49,602
|
41,894
|
7,708
|
|
||||
|
SOCIO-DEMOGRAPHIC FACTORS
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
Age Group
|
|
|
|
|
|
|
|
p<0.0001
|
|
Younger than 15
|
3,209
|
2,990
|
7.1%
|
93.2%
|
219
|
2.8%
|
6.8%
|
|
|
15 to 24
|
11,233
|
10,005
|
23.9%
|
89.1%
|
1,228
|
15.9%
|
10.9%
|
|
|
25 to 34
|
9,402
|
8,002
|
19.1%
|
85.1%
|
1,400
|
18.2%
|
14.9%
|
|
|
35 to 44
|
8,297
|
6,725
|
16.1%
|
81.1%
|
1,572
|
20.4%
|
18.9%
|
|
|
45 to 54
|
6,920
|
5,482
|
13.1%
|
79.2%
|
1,438
|
18.7%
|
20.8%
|
|
|
55 to 64
|
4,771
|
3,820
|
9.1%
|
80.1%
|
951
|
12.4%
|
19.9%
|
|
|
65 to 74
|
2,859
|
2,347
|
5.6%
|
82.1%
|
512
|
6.7%
|
17.9%
|
|
|
75 and older
|
2,895
|
2,512
|
6.0%
|
86.8%
|
383
|
5.0%
|
13.2%
|
|
|
|
|
|
|
|
|
|
|
|
|
Gender
|
|
|
|
|
|
|
|
p<0.0001
|
|
Female
|
23,595
|
20,319
|
48.5%
|
86.1%
|
3,276
|
42.5%
|
13.9%
|
|
|
Male
|
25,988
|
21,559
|
51.5%
|
83.0%
|
4,429
|
57.5%
|
17.0%
|
|
|
|
|
|
|
|
|
|
|
|
|
Interpreter Used
|
|
|
|
|
|
|
|
p<0.0001
|
|
No
|
49,206
|
41,774
|
99.7%
|
84.9%
|
7,432
|
96.4%
|
15.1%
|
|
|
Yes
|
396
|
120
|
0.3%
|
30.3%
|
276
|
3.6%
|
69.7%
|
|
|
|
|
|
|
|
|
|
|
|
|
Prior Claim
|
|
|
|
|
|
|
|
p<0.0001
|
|
No
|
48,886
|
41,382
|
98.8%
|
84.7%
|
7,504
|
97.4%
|
15.3%
|
|
|
Yes
|
716
|
512
|
1.2%
|
71.5%
|
204
|
2.6%
|
28.5%
|
|
|
|
|
|
|
|
|
|
|
|
|
Remoteness
|
|
|
|
|
|
|
|
p<0.001
|
|
Major Cities of Victoria
|
35,959
|
30,439
|
73.5%
|
84.6%
|
5,520
|
72.7%
|
15.4%
|
|
|
Inner Regional Victoria
|
10,837
|
9,174
|
22.2%
|
84.7%
|
1,663
|
21.9%
|
15.3%
|
|
|
Outer Regional, Remote, and Very Remote Victoria
|
2,222
|
1,809
|
4.3%
|
81.4%
|
413
|
5.4%
|
18.6%
|
|
|
|
|
|
|
|
|
|
|
|
|
SES: IRSAD State Decile
|
|
|
|
|
|
|
|
p<0.0001
|
|
Decile 1
|
6,455
|
5,326
|
12.8%
|
82.5%
|
1,129
|
14.9%
|
17.5%
|
|
|
Decile 2
|
3,166
|
2,600
|
6.3%
|
82.1%
|
566
|
7.4%
|
17.9%
|
|
|
Decile 3
|
3,585
|
2,975
|
7.2%
|
83.0%
|
610
|
8.0%
|
17.0%
|
|
|
Decile 4
|
4,777
|
3,966
|
9.6%
|
83.0%
|
811
|
10.7%
|
17.0%
|
|
|
Decile 5
|
5,244
|
4,389
|
10.6%
|
83.7%
|
855
|
11.2%
|
16.3%
|
|
|
Decile 6
|
4,339
|
3,635
|
8.8%
|
83.8%
|
704
|
9.3%
|
16.2%
|
|
|
Decile 7
|
4,964
|
4,236
|
10.2%
|
85.3%
|
728
|
9.6%
|
14.7%
|
|
|
Decile 8
|
4,668
|
3,990
|
9.6%
|
85.5%
|
678
|
8.9%
|
14.5%
|
|
|
Decile 9
|
7,294
|
6,329
|
15.3%
|
86.8%
|
965
|
12.7%
|
13.2%
|
|
|
Decile 10
|
4,580
|
4,022
|
9.7%
|
87.8%
|
558
|
7.3%
|
12.2%
|
|
|
|
|
|
|
|
|
|
|
|
|
CRASH FACTORS
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
Number of Vehicles in Crash
|
|
|
|
|
|
|
|
p<0.0001
|
|
Single Vehicle Crash
|
19,669
|
16,412
|
39.6%
|
83.4%
|
3,257
|
42.6%
|
16.6%
|
|
|
Multi Vehicle Crash
|
29,442
|
25,047
|
60.4%
|
85.1%
|
4,395
|
57.4%
|
14.9%
|
|
|
|
|
|
|
|
|
|
|
|
|
Claimant Road User Group
|
|
|
|
|
|
|
|
p<0.0001
|
|
Driver
|
23,259
|
20,312
|
48.5%
|
87.3%
|
2,947
|
38.2%
|
12.7%
|
|
|
Passenger
|
10,612
|
9,127
|
21.8%
|
86.0%
|
1,485
|
19.3%
|
14.0%
|
|
|
Motorcyclist
|
6,100
|
4,968
|
11.9%
|
81.4%
|
1,132
|
14.7%
|
18.6%
|
|
|
Pedestrian
|
4,211
|
2,839
|
6.8%
|
67.4%
|
1,372
|
17.8%
|
32.6%
|
|
|
Cyclist
|
2,768
|
2,367
|
5.7%
|
85.5%
|
401
|
5.2%
|
14.5%
|
|
|
Train/Tram
|
202
|
143
|
0.3%
|
70.8%
|
59
|
0.8%
|
29.2%
|
|
|
Unknown
|
2,450
|
2,138
|
5.1%
|
87.3%
|
312
|
4.1%
|
12.7%
|
|
|
|
|
|
|
|
|
|
|
|
|
INJURY FACTORS
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
Injury Type
|
|
|
|
|
|
|
|
p<0.0001
|
|
Catastrophic
|
266
|
31
|
0.1%
|
11.7%
|
235
|
3.1%
|
88.3%
|
|
|
Musculoskeletal - Whiplash
|
15,515
|
13,860
|
33.1%
|
89.3%
|
1,655
|
21.5%
|
10.7%
|
|
|
Musculoskeletal - Sprains and Strains
|
3,441
|
3,187
|
7.6%
|
92.6%
|
254
|
3.3%
|
7.4%
|
|
|
Orthopaedic - Limb Fractures
|
5,884
|
4,291
|
10.2%
|
72.9%
|
1,593
|
20.7%
|
27.1%
|
|
|
Orthopaedic - Other Fractures
|
3,002
|
2,448
|
5.8%
|
81.5%
|
554
|
7.2%
|
18.5%
|
|
|
Orthopaedic - Dislocations
|
994
|
719
|
1.7%
|
72.3%
|
275
|
3.6%
|
27.7%
|
|
|
Other Injuries - Abrasions, Contusions, and Lacerations
|
8,454
|
8,012
|
19.1%
|
94.8%
|
442
|
5.7%
|
5.2%
|
|
|
Other Injuries - Other
|
5,579
|
4,767
|
11.4%
|
85.4%
|
812
|
10.5%
|
14.6%
|
|
|
Other Serious Injuries - Mild Acquired Brain Injury
|
3,139
|
2,264
|
5.4%
|
72.1%
|
875
|
11.4%
|
27.9%
|
|
|
Other Serious Injuries - Internal Injuries
|
2,528
|
1,818
|
4.3%
|
71.9%
|
710
|
9.2%
|
28.1%
|
|
|
Other Serious Injuries - Other
|
800
|
497
|
1.2%
|
62.1%
|
303
|
3.9%
|
37.9%
|
|
|
|
|
|
|
|
|
|
|
|
|
Length of Hospital Stay
|
|
|
|
|
|
|
|
p<0.0001
|
|
0 Days^
|
30,809
|
28,095
|
67.1%
|
91.2%
|
2,714
|
35.2%
|
8.8%
|
|
|
1 Days
|
8,496
|
7,733
|
18.5%
|
91.0%
|
763
|
9.9%
|
9.0%
|
|
|
2–7 Days
|
5,855
|
4,299
|
10.3%
|
73.4%
|
1,556
|
20.2%
|
26.6%
|
|
|
More Than 7 Days
|
4,442
|
1,767
|
4.2%
|
39.8%
|
2,675
|
34.7%
|
60.2%
|
|
|
|
|
|
|
|
|
|
|
|
|
EARLY RECOVERY OUTCOMES (THREE MONTHS POST-CRASH)
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
Work Disability (Three Months Post-Crash)#
|
|
|
|
|
|
|
|
p<0.0001
|
|
No
|
39,721
|
36,255
|
86.5%
|
91.3%
|
3,466
|
45.0%
|
8.7%
|
|
|
Yes
|
9,881
|
5,639
|
13.5%
|
87.1%
|
4,242
|
55.0%
|
42.9%
|
|
|
|
|
|
|
|
|
|
|
|
|
Mental Health Indicators (Three Months Post-Crash)
|
|
|
|
|
|
|
|
p<0.0001
|
|
No
|
40,795
|
37,064
|
88.5%
|
90.9%
|
3,731
|
48.4%
|
9.1%
|
|
|
Yes
|
8,807
|
4,830
|
11.5%
|
54.8%
|
3,977
|
51.6%
|
45.2%
|
|
|
|
|
|
|
|
|
|
|
|
|
Pain Indicators (Three Months Post-Crash)
|
|
|
|
|
|
|
|
p<0.0001
|
|
No
|
42,458
|
37,488
|
89.5%
|
88.3%
|
4,970
|
64.5%
|
11.7%
|
|
|
Yes
|
7,144
|
4,406
|
10.5%
|
61.7%
|
2,738
|
35.5%
|
38.3%
|
|
|
|
|
|
|
|
|
|
|
|
|
LONG TERM RECOVERY OUTCOMES (ONE YEAR POST-CRASH)
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
Work Disability (One Year Post-Crash)#
|
|
|
|
|
|
|
|
p<0.0001
|
|
No
|
40,958
|
37,141
|
88.7%
|
90.7%
|
3,817
|
49.5%
|
9.3%
|
|
|
Yes
|
8,644
|
4,753
|
11.3%
|
55.0%
|
3,891
|
50.5%
|
45.0%
|
|
|
|
|
|
|
|
|
|
|
|
|
Mental Health Indicators (One Year Post-Crash)
|
|
|
|
|
|
|
|
p<0.0001
|
|
No
|
41,178
|
37,303
|
89.0%
|
90.6%
|
3,875
|
50.3%
|
9.4%
|
|
|
Yes
|
8,424
|
4,591
|
11.0%
|
54.5%
|
3,833
|
49.7%
|
45.5%
|
|
|
|
|
|
|
|
|
|
|
|
|
Pain Indicators (One Year Post-Crash)
|
|
|
|
|
|
|
|
p<0.0001
|
|
No
|
42,615
|
37,588
|
89.7%
|
88.2%
|
5,027
|
65.2%
|
11.8%
|
|
|
Yes
|
6,987
|
4,306
|
10.3%
|
61.6%
|
2,681
|
34.8%
|
38.4%
|
|
|
|
|
|
|
|
|
|
|
|
|
^ As length of hospital stay was calculated based on inpatient admissions,
this category includes claimants who did not attend hospital,
as well as
claimants with ED presentations and/or outpatient admissions only.
# Some claimants were not working at the time of the
crash (for example, because they were below the minimum working age, unemployed,
or retired) and were thus ineligible for work disability payments. As a result,
the ‘No’ category includes both claimants
who were and were not
eligible for work disability.
|
||||||||
For claimants who were hospitalised, the modelled associations between the socio-demographic, crash, injury, and recovery indicators and lawyer use within six years post-crash are shown in Table 2 (N=16,322). Injury severity explained 8.8% of the variation in lawyer use when entered into a logistic regression alone (result not shown in Table 2). The socio-demographic, crash, and injury variables that were significantly associated with lawyer use were age, prior claiming, SES, number of vehicles involved in the crash, claimant road user group, and injury type (Model One); neither gender nor remoteness were statistically significant in the adjusted model. Model One explained 11.7% of the variation in lawyer use (entering these variables into logistic regressions separately revealed that the socio-demographic and crash variables contributed 4.2% of this, whilst injury type contributed the remaining 7.5%). Adding injury severity increased the amount of variation explained to 16.5% (Model Two). Adding the number of negative recovery outcomes experienced at 3 (Model Three) or 12 (Model Four) months post-crash substantially increased the amount of variation explained to 39.4% and 39.6%, respectively.
The odds of lawyer use tended to be significantly lower among claimants who were young (below 25), were socio-economically advantaged, and sustained injuries in the ‘other injuries’ categories (see Figure 2). In contrast, the odds of lawyer use tended to be significantly higher for claimants who had prior claims, were involved in multi-vehicle crashes, were passengers, pedestrians or cyclists at the time of the crash, sustained injuries in the ‘orthopaedic’ (limb fractures and dislocations) and ‘other serious injuries’ categories, and sustained more severe injuries. The odds of lawyer use were also significantly higher for claimants who were experiencing one or more negative recovery outcomes at 3 or 12 months post-crash.
Table 2: Associations between Socio-Demographic, Crash, Injury, and Recovery Variables and Lawyer Use in the Hospitalised Cohort
|
Variable
|
Model 1 a
OR [95% CI]
|
Model 2 b
OR [95% CI]
|
Model 3 c
OR [95% CI]
|
Model 4 d
OR [95% CI]
|
|
SOCIO-DEMOGRAPHIC FACTORS
|
||||
|
|
|
|
|
|
|
Age Group (ref=35 to 44)
|
|
|
|
|
|
Younger than 15
|
0.30 [0.24 – 0.39]
|
0.30 [0.23 – 0.38]
|
0.36 [0.27 – 0.48]
|
0.33 [0.24 – 0.44]
|
|
15 to 24
|
0.57 [0.50 – 0.64]
|
0.54 [0.48 – 0.61]
|
0.67 [0.58 – 0.78]
|
0.66 [0.57 – 0.77]
|
|
25 to 34
|
0.77 [0.68 – 0.87]
|
0.75 [0.66 – 0.85]
|
0.86 [0.74 – 1.01]
|
0.88 [0.76 – 1.03]
|
|
45 to 54
|
1.04 [0.91 – 1.18]
|
1.04 [0.91 – 1.19]
|
1.03 [0.87 – 1.21]
|
1.06 [0.91 – 1.25]
|
|
55 to 64
|
0.92 [0.79 – 1.07]
|
0.90 [0.77 – 1.04]
|
1.03 [0.86 – 1.24]
|
1.04 [0.87 – 1.25]
|
|
65 to 74
|
0.87 [0.73 – 1.04]
|
0.84 [0.70 – 1.00]
|
1.36 [1.10 – 1.68]
|
1.30 [1.06 – 1.61]
|
|
75 and older
|
0.54 [0.46 – 0.65]
|
0.47 [0.39 – 0.56]
|
1.09 [0.88 – 1.34]
|
0.96 [0.78 – 1.18]
|
|
|
|
|
|
|
|
Gender (ref=Male)
|
|
|
|
|
|
Female
|
1.01 [0.93 – 1.10]
|
1.09 [1.00 – 1.19]
|
0.96 [0.87 – 1.07]
|
0.94 [0.85 – 1.05]
|
|
|
|
|
|
|
|
Prior Claim (ref=No)
|
|
|
|
|
|
Yes
|
1.57 [1.17 – 2.10]
|
1.62 [1.20 – 2.19]
|
1.53 [1.07 – 2.19]
|
1.47 [1.02 – 2.12]
|
|
|
|
|
|
|
|
Remoteness (ref=Major Cities of Victoria)
|
|
|
|
|
|
Inner Regional Victoria
|
1.09 [0.99 – 1.21]
|
1.04 [0.94 – 1.15]
|
0.98 [0.87 – 1.11]
|
0.97 [0.86 – 1.09]
|
|
Outer Regional, Remote, and Very Remote Victoria
|
1.03 [0.85 – 1.24]
|
0.96 [0.79 – 1.16]
|
0.96 [0.76 – 1.20]
|
0.88 [0.70 – 1.11]
|
|
|
|
|
|
|
|
SES: IRSAD State Decile (ref=Deciles 5 and 6)
|
|
|
|
|
|
Deciles 1 and 2
|
1.12 [0.99 – 1.26]
|
1.12 [0.99 – 1.27]
|
1.16 [1.01 – 1.35]
|
1.17 [1.01 – 1.35]
|
|
Deciles 3 and 4
|
1.06 [0.93 – 1.19]
|
1.04 [0.91 – 1.18]
|
0.99 [0.85 – 1.15]
|
1.00 [0.86 – 1.16]
|
|
Deciles 7 and 8
|
0.89 [0.79 – 1.00]
|
0.88 [0.78 – 1.00]
|
0.90 [0.78 – 1.04]
|
0.91 [0.79 – 1.05]
|
|
Deciles 9 and 10
|
0.73 [0.64 – 0.82]
|
0.71 [0.63 – 0.80]
|
0.72 [0.62 – 0.83]
|
0.72 [0.63 – 0.84]
|
|
|
|
|
|
|
|
CRASH FACTORS
|
||||
|
|
|
|
|
|
|
Number of Vehicles in Crash (ref=Single Vehicle Crash)
|
|
|
|
|
|
Multi Vehicle Crash
|
1.52 [1.40 – 1.65]
|
1.57 [1.44 – 1.71]
|
1.77 [1.60 – 1.96]
|
1.68 [1.52 – 1.85]
|
|
|
|
|
|
|
|
Claimant Road User Group (ref=Driver)
|
|
|
|
|
|
Passenger
|
1.96 [1.76 – 2.18]
|
1.95 [1.75 – 2.18]
|
2.08 [1.82 – 2.36]
|
2.00 [1.75 – 2.27]
|
|
Motorcyclist
|
1.15 [1.02 – 1.29]
|
1.18 [1.05 – 1.33]
|
1.12 [0.98 – 1.30]
|
1.11 [0.96 – 1.28]
|
|
Pedestrian
|
2.88 [2.53 – 3.28]
|
2.76 [2.41 – 3.16]
|
3.37 [2.87 – 3.95]
|
3.23 [2.76 – 3.78]
|
|
Cyclist
|
1.37 [1.15 – 1.63]
|
1.46 [1.22 – 1.75]
|
2.18 [1.77 – 2.69]
|
2.00 [1.63 – 2.45]
|
|
Unknown
|
1.08 [0.85 – 1.38]
|
1.13 [0.88 – 1.45]
|
1.44 [1.08 – 1.92]
|
1.40 [1.05 – 1.87]
|
|
|
|
|
|
|
|
INJURY FACTORS
|
||||
|
|
|
|
|
|
|
Injury Type (ref=Musculoskeletal – Whiplash)
|
|
|
|
|
|
Musculoskeletal – Strains and Sprains
|
1.13 [0.84 – 1.52]
|
1.11 [0.82 – 1.50]
|
1.19 [0.84 – 1.67]
|
1.28 [0.91 – 1.81]
|
|
Orthopaedic – Limb Fractures
|
3.83 [3.26 – 4.50]
|
2.58 [2.18 – 3.06]
|
2.30 [1.88 – 2.81]
|
2.59 [2.13 – 3.16]
|
|
Orthopaedic – Other Fractures
|
2.25 [1.88 – 2.69]
|
1.11 [0.92 – 1.35]
|
1.17 [0.93 – 1.46]
|
1.23 [0.99 – 1.55]
|
|
Orthopaedic – Dislocations
|
3.46 [2.66 – 4.49]
|
3.30 [2.53 – 4.30]
|
2.30 [1.68 – 3.16]
|
2.38 [1.73 – 3.26]
|
|
Other Injuries – Abrasions, Contusions, and Lacerations
|
0.62 [0.51 – 0.75]
|
0.50 [0.41 – 0.61]
|
0.67 [0.54 – 0.85]
|
0.69 [0.55 – 0.87]
|
|
Other Injuries – Other
|
0.55 [0.41 – 0.75]
|
0.38 [0.28 – 0.52]
|
0.54 [0.38 – 0.76]
|
0.55 [0.39 – 0.78]
|
|
Other Serious Injuries – Mild Acquired Brain Injury
|
4.42 [3.74 – 5.24]
|
1.56 [1.29 – 1.89]
|
1.32 [1.05 – 1.65]
|
1.41 [1.12 – 1.77]
|
|
Other Serious Injuries – Internal Injuries
|
4.26 [3.57 – 5.07]
|
1.34 [1.10 – 1.63]
|
1.31 [1.04 – 1.66]
|
1.36 [1.08 – 1.72]
|
|
Other Serious Injuries – Other
|
5.45 [4.37 – 6.80]
|
2.71 [2.14 – 3.43]
|
2.21 [1.67 – 2.93]
|
2.36 [1.77 – 3.13]
|
|
|
|
|
|
|
|
INJURY SEVERITY
|
||||
|
|
|
|
|
|
|
ICISS Score (ref=Quartile 1 – Least Severe Injuries)
|
|
|
|
|
|
Quartile 2
|
-
|
1.32 [1.15 – 1.50]
|
1.16 [1.00 – 1.35]
|
1.16 [1.00 – 1.35]
|
|
Quartile 3
|
-
|
1.94 [1.71 – 2.20]
|
1.48 [1.28 – 1.72]
|
1.54 [1.33 – 1.78]
|
|
Quartile 4 – Most Severe Injuries
|
-
|
5.14 [4.48 – 5.89]
|
2.99 [2.55 – 3.51]
|
3.38 [2.88 – 3.96]
|
|
|
|
|
|
|
|
EARLY RECOVERY OUTCOMES (THREE MONTHS POST-CRASH)
|
||||
|
|
|
|
|
|
|
Number of Short-Term Recovery Outcomes Experienced (ref=None)
|
|
|
|
|
|
One – Short-Term Work Disability Only
|
-
|
-
|
4.90 [4.24 – 5.66]
|
-
|
|
One – Short-Term Mental Health Indicators Only
|
-
|
-
|
10.71 [8.52 – 13.48]
|
-
|
|
One – Short-Term Pain Indicators Only
|
-
|
-
|
5.97 [4.13 – 8.63]
|
-
|
|
Two
|
-
|
-
|
21.69 [18.27 – 25.76]
|
-
|
|
Three
|
-
|
-
|
24.70 [21.43 – 28.47]
|
-
|
|
|
|
|
|
|
|
LONG-TERM RECOVERY OUTCOMES (ONE YEAR POST-CRASH)
|
||||
|
|
|
|
|
|
|
Number of Long-Term Recovery Outcomes Experienced (ref=None)
|
|
|
|
|
|
One – Long-Term Work Disability Only
|
-
|
-
|
-
|
8.23 [6.73 – 10.07]
|
|
One – Long-Term Mental Health Indicators Only
|
-
|
-
|
-
|
16.68 [12.42 – 22.39]
|
|
One – Long-Term Pain Indicators Only
|
-
|
-
|
-
|
7.88 [4.78 – 13.00]
|
|
Two
|
-
|
-
|
-
|
23.12 [19.03 – 28.10]
|
|
Three
|
-
|
-
|
-
|
21.11 [18.34 – 24.30]
|
a Model 1: The Link Test (p=.825) suggested no statistically significant departure from model adequacy. The Tjur R2 value was 0.1171.
b Model 2: The Link Test (p=.432) suggested no statistically significant departure from model adequacy. The Tjur R2 value was 0.1649.
c Model 3: The Link Test (p=<0.001) suggested that there was a statistically significant departure from model adequacy.[75] The Tjur R2 value was 0.3938.
d Model 4: The Link Test (p=<0.001) suggested that there was a statistically significant departure from model adequacy. The Tjur R2 value was 0.3959
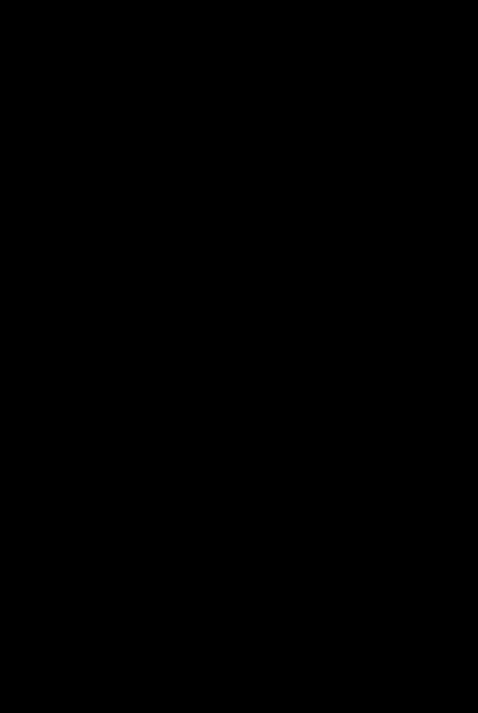
Figure 2: Significant Associations with Lawyer Use in the Hospitalised Context
For the non-hospitalised cohort, the modelled associations between the socio-demographic, crash, injury, and recovery indicators and lawyer use within six years post-crash are shown in Table 3 (N=31,703). Entering the socio-demographic, crash, and injury factors into a logistic regression alone (Model One) indicated that, in contrast to the hospitalised cohort, all variables (age, gender, prior claiming, remoteness, SES, number of vehicles involved in the crash, claimant road user group, and injury type) were significantly associated with lawyer use. Model One explained 9.0% of the variation in lawyer use (entering these variables into logistic regressions separately revealed that the socio-demographic and crash variables contributed 6.5% of this, whilst injury type contributed the remaining 2.5%). Adding the number of negative recovery outcomes experienced at 3 (Model Two) or 12 (Model Three) months post-crash substantially increased the amount of variation explained to 17.2% and 18.0%, respectively.
In the non-hospitalised group, the odds of lawyer use tended to be significantly lower among claimants who were aged below 35 years or above 75 years, were female, were socio-economically advantaged, were motorcyclists, and sustained injuries in the ‘musculoskeletal’, ‘other injuries’ (abrasions, contusions, lacerations) and ‘other serious injuries’ (mild acquired brain injury) categories (see Figure 3). In contrast, the odds of lawyer use tended to be higher for claimants who were aged 45 to 64 years, had prior claims, lived in outer regional, remote and very remote Victoria, were socio-economically disadvantaged, were involved in multi-vehicle crashes, were passengers or pedestrians, and sustained injuries in the ‘orthopaedic’ (dislocations) and ‘other serious injuries’ (other) categories. The odds of lawyer use were also significantly higher for claimants who experienced one or more negative recovery outcomes at 3 or 12 months post-crash.
Table 3: Associations between Socio-Demographic, Crash, Injury, and Recovery Variables and Lawyer Use in the Non-Hospitalised Cohort
|
Variable
|
Model 1 a
OR [95% CI]
|
Model 2 b
OR [95% CI]
|
Model 3 c
OR [95% CI]
|
|
SOCIO-DEMOGRAPHIC FACTORS
|
|||
|
|
|
|
|
|
Age Group (ref=35 to 44)
|
|
|
|
|
Younger than 15
|
0.24 [0.19 – 0.30]
|
0.26 [0.20 – 0.33]
|
0.25 [0.19 – 0.32]
|
|
15 to 24
|
0.34 [0.30 – 0.40]
|
0.41 [0.35 – 0.47]
|
0.40 [0.34 – 0.46]
|
|
25 to 34
|
0.68 [0.60 – 0.77]
|
0.73 [0.64 – 0.83]
|
0.72 [0.63 – 0.82]
|
|
45 to 54
|
1.25 [1.11 – 1.41]
|
1.22 [1.08 – 1.39]
|
1.20 [1.06 – 1.36]
|
|
55 to 64
|
1.18 [1.03 – 1.35]
|
1.23 [1.07 – 1.42]
|
1.22 [1.06 – 1.40]
|
|
65 to 74
|
0.79 [0.67 – 0.95]
|
0.91 [0.76 – 1.10]
|
0.88 [0.73 – 1.06]
|
|
75 and older
|
0.39 [0.31 – 0.50]
|
0.50 [0.40 – 0.64]
|
0.49 [0.39 – 0.63]
|
|
|
|
|
|
|
Gender (ref=Male)
|
|
|
|
|
Female
|
0.78 [0.72 – 0.84]
|
0.79 [0.72 – 0.86]
|
0.78 [0.72 – 0.85]
|
|
|
|
|
|
|
Prior Claim (ref=No)
|
|
|
|
|
Yes
|
2.85 [2.27 – 3.58]
|
2.73 [2.14 – 3.49]
|
2.74 [2.15 – 3.49]
|
|
|
|
|
|
|
Remoteness (ref=Major Cities of Victoria)
|
|
|
|
|
Inner Regional Victoria
|
0.90 [0.81 – 0.99]
|
0.97 [0.87 – 1.08]
|
0.96 [0.86 – 1.07]
|
|
Outer Regional, Remote, and Very Remote Victoria
|
1.25 [1.05 – 1.49]
|
1.29 [1.07 – 1.54]
|
1.26 [1.05 – 1.51]
|
|
|
|
|
|
|
SES: IRSAD State Decile (ref=Deciles 5 and 6)
|
|
|
|
|
Deciles 1 and 2
|
1.14 [1.01 – 1.28]
|
1.19 [1.05 – 1.34]
|
1.19 [1.05 – 1.34]
|
|
Deciles 3 and 4
|
1.02 [0.90 – 1.15]
|
1.04 [0.91 – 1.19]
|
1.05 [0.92 – 1.20]
|
|
Deciles 7 and 8
|
0.77 [0.68 – 0.88]
|
0.80 [0.70 – 0.92]
|
0.81 [0.71 – 0.92]
|
|
Deciles 9 and 10
|
0.64 [0.57 – 0.73]
|
0.65 [0.57 – 0.74]
|
0.64 [0.57 – 0.73]
|
|
|
|
|
|
|
CRASH FACTORS
|
|||
|
|
|
|
|
|
Number of Vehicles in Crash (ref=Single Vehicle Crash)
|
|
|
|
|
Multi Vehicle Crash
|
1.27 [1.16 – 1.39]
|
1.32 [1.20 – 1.46]
|
1.32 [1.20 – 1.45]
|
|
|
|
|
|
|
Claimant Road User Group (ref=Driver)
|
|
|
|
|
Passenger
|
1.19 [1.07 – 1.33]
|
1.25 [1.11 – 1.40]
|
1.25 [1.12 – 1.41]
|
|
Motorcyclist
|
0.63 [0.53 – 0.74]
|
0.70 [0.59 – 0.84]
|
0.73 [0.61 – 0.87]
|
|
Pedestrian
|
5.03 [4.43 – 5.71]
|
5.08 [4.43 – 5.82]
|
4.99 [4.35 – 5.72]
|
|
Cyclist
|
1.05 [0.86 – 1.27]
|
1.12 [0.92 – 1.37]
|
1.09 [0.89 – 1.33]
|
|
Unknown
|
1.12 [0.93 – 1.36]
|
0.90 [0.74 – 1.10]
|
0.92 [0.75 – 1.12]
|
|
|
|
|
|
|
INJURY FACTORS
|
|||
|
|
|
|
|
|
Injury Type (ref=Musculoskeletal – Whiplash)
|
|
|
|
|
Musculoskeletal – Strains and Sprains
|
0.49 [0.41 – 0.58]
|
0.54 [0.45 – 0.65]
|
0.55 [0.46 – 0.66]
|
|
Orthopaedic – Limb Fractures
|
1.18 [1.00 – 1.40]
|
1.15 [0.96 – 1.37]
|
1.27 [1.06 – 1.52]
|
|
Orthopaedic – Other Fractures
|
1.01 [0.83 – 1.24]
|
1.03 [0.83 – 1.27]
|
1.09 [0.88 – 1.35]
|
|
Orthopaedic – Dislocations
|
3.27 [2.62 – 4.09]
|
2.66 [2.10 – 3.38]
|
3.06 [2.41 – 3.89]
|
|
Other Injuries – Abrasions, Contusions, and Lacerations
|
0.34 [0.29 – 0.40]
|
0.42 [0.35 – 0.49]
|
0.42 [0.36 – 0.49]
|
|
Other Injuries – Other
|
1.32 [1.19 – 1.47]
|
1.07 [0.95 – 1.20]
|
1.07 [0.95 – 1.21]
|
|
Other Serious Injuries – Mild Acquired Brain Injury
|
0.71 [0.55 – 0.90]
|
0.73 [0.57 – 0.95]
|
0.73 [0.57 – 0.95]
|
|
Other Serious Injuries – Internal Injuries
|
1.05 [0.83 – 1.33]
|
1.15 [0.89 – 1.47]
|
1.16 [0.90 – 1.49]
|
|
Other Serious Injuries – Other
|
3.69 [2.65 – 5.13]
|
3.13 [2.18 – 4.49]
|
3.41 [2.38 – 4.89]
|
|
|
|
|
|
|
EARLY RECOVERY OUTCOMES (THREE MONTHS POST-CRASH)
|
|||
|
|
|
|
|
|
Number of Short-Term Recovery Outcomes Experienced (ref=None)
|
|
|
|
|
One – Short-Term Work Disability Only
|
-
|
6.15 [5.04 – 7.51]
|
-
|
|
One – Short-Term Mental Health Indicators Only
|
-
|
18.20 [14.33 – 23.13]
|
-
|
|
One – Short-Term Pain Indicators Only
|
-
|
11.37 [6.33 – 20.40]
|
-
|
|
Two or Three
|
-
|
5.14 [4.71 – 5.61]
|
-
|
|
|
|
|
|
|
LONG-TERM RECOVERY OUTCOMES (ONE YEAR POST-CRASH)
|
|||
|
|
|
|
|
|
Number of Long-Term Recovery Outcomes Experienced (ref=None)
|
|
|
|
|
One – Long-Term Work Disability Only
|
-
|
-
|
13.71 [10.34 – 18.17]
|
|
One – Long-Term Mental Health Indicators Only
|
-
|
-
|
28.14 [20.91 – 37.86]
|
|
One – Long-Term Pain Indicators Only
|
-
|
-
|
17.23 [9.67 – 30.71]
|
|
Two or Three
|
-
|
-
|
5.04 [4.62 – 5.50]
|
|
|
|
|
|
|
a Model 1: The Link Test (p=.694) suggested no
statistically significant departure from model adequacy. The Tjur
R2 value was 0.0897.
b Model 2: The Link Test (p=<0.001) suggested
that there was a statistically significant departure from model
adequacy.[76] The Tjur
R2 value was 0.1719.
c Model 3: The Link Test (p=<0.001) suggested
that there was a statistically significant departure from model adequacy. The
Tjur R2 value was 0.1800.
|
|||

Figure 3: Significant Associations with Lawyer Use in the Non-Hospitalised Context
Although injury severity and other individual-level socio-demographic, crash, and injury factors played a role in explaining claimant engagement of lawyers, recovery outcomes had by far the greatest impact. In both cohorts, claimants who had prior claims, were relatively socio-economically disadvantaged, were injured in multi-vehicle crashes, were passengers or pedestrians, sustained ‘orthopaedic’ (limb fractures and dislocations) and ‘other serious’ (other) injuries, or who experienced one or more negative recovery outcomes had a relatively high likelihood of engaging a lawyer. Claimants who were young (below 25), were relatively socio-economically advantaged, and sustained ‘other’ (abrasion, contusion, and laceration) injuries had a relatively low likelihood of engaging a lawyer.
In Australia, studies conducted among individuals with all types of legal problems suggest that some individuals are less likely to seek advice (including legal advice) in response to these problems;[77] for example, those who are young (ie, aged 15 to 34), male, not disabled, not single parents, speak a main language other than English, and have markers of socio-economic disadvantage.[78] Several of these groups are also particularly vulnerable to experiencing multiple and substantial legal problems (including those who are young and have markers of socio-economic disadvantage)[79] and failing to finalise these problems (including those who speak a main language other than English and have markers of socio-economic disadvantage).[80]
In terms of age, our findings were similar to those of studies of legal problems more generally in that, in both cohorts, younger claimants (ie, those below 25) had lower odds of engaging lawyers. There are a number of potential explanations for this relationship in the TAC scheme. First, in this scheme, children are reliant on their parents to instigate and pursue claims on their behalf. If a child is injured due to their parents’ driving, there might be a natural reluctance on the part of that parent to pursue a claim because of their responsibility for the crash. Although the TAC would indemnify the parent so that they would not have to pay damages directly, the parent might be unaware of this or concerned that they would still be held responsible.
Second, the timelines for claiming impairment lump sum and common law benefits are extended for children in the TAC scheme. A child’s degree of impairment is assessed when they reach the age of 18 years if their injuries have stabilised by that time.[81] Children also have six years from the date they turn 18 to lodge a common law claim, as prior to that they are under a ‘legal disability’.[82] As a result, some young people who did not use legal services in the follow-up period in this study might still use these services once they come of age to claim impairment lump sum or common law benefits themselves.
Finally, there is a general tendency for young people not to recognise that their problems have a legal dimension or potential legal solution, and to lack awareness about accessible legal services.[83] Young people can also be reluctant to engage legal services, and struggle to participate in legal processes.[84]
Notably, our findings differed from those of a study conducted in a different Australian compensation scheme, in which age was not associated with lawyer use.[85] This may be because that study focused on whiplash claimants in the NSW scheme, and factors associated with lawyer use might differ across injury types or compensation scheme designs. Injury profile might also differ across age groups, and so the age distribution of the sample in that study might differ from that in the current study.
The findings for the negative recovery outcomes were also similar to those of studies of legal problems more generally, which indicate that individuals with physical and mental ill-health are more likely to both engage legal services and fail to finalise their problems within a short timeframe, perhaps because their problems are particularly complex or severe, or because they lack the capacity to finalise their problems alone. In studies of individuals with road traffic injuries, it has been suggested that lawyer use itself causes physical and mental ill-health and delayed return to work. A number of studies have explored stressful aspects of legal processes that could explain this relationship, such as the need to relive the initial crash,[86] prove an injury or disability in the face of explicit doubts,[87] and expose intensely private information to public view.[88] However, less attention has been paid to the role of lawyers themselves, although they are frequently portrayed as adversarial parties who exacerbate an already harmful process by adding complexity to cases and prolonging conflict and strife.[89]
Notably, studies of individuals with road traffic injuries have generally failed to find evidence of a causal link between lawyer use and recovery outcomes, such as return to work, once variables that could predict both lawyer use and recovery outcomes are adjusted for.[90] Indeed, the current study suggests that the proposed link might be reversed, and that injured persons might engage lawyers when they experience delays returning to work, or mental health or pain issues. In compensation settings, these issues could impair claimants’ ability to navigate schemes alone; complicate claimants’ treatment needs, leading to disputes over access to benefits; and impair claimants’ personal and social functioning, leading to higher perceived injury severity and the pursuit of impairment lump sum and common law benefits, all of which can necessitate the engagement of lawyers.
Our findings for SES differed from those of studies of legal problems more generally. In those studies, individuals who had markers of socio-economic disadvantage were unlikely to seek legal advice[91] or finalise problems in the absence of this advice.[92] Conversely, in the current study, socio-economically disadvantaged claimants were highly likely to use legal services. This might be because, for problems other than personal injuries, socio-economically disadvantaged persons often cannot afford to pay for legal services outright and are instead reliant on the availability of legal aid and community legal centre (‘CLC’) services.[93] The amount of legal aid provided is often woefully inadequate, and there have been substantial budget cuts in the CLC sector in recent years that have reduced the availability of services and made it harder for socio-economically disadvantaged persons to receive legal assistance.[94] For personal injuries, however, legal services tend to be available on a ‘no win, no fee’ basis, which removes cost barriers for socio-economically disadvantaged claimants and increases lawyer use.
Alternatively, it might be that individuals who are socio-economically advantaged have higher legal capability than those who are not, where legal capability is defined as the legal knowledge and skills needed to pursue a legal resolution, and psychological readiness to act until this resolution is achieved.[95] Outside personal injury compensation schemes, this imbalance in legal capability manifests as a tendency toward inaction and away from lawyer use in disadvantaged groups, and away from inaction and toward lawyer use in advantaged groups.[96] However, this study suggests that in personal injury compensation schemes, the reverse might be true. This might be because claimants with high legal capability can navigate compensation schemes and finalise problems without legal intervention, whilst those with low legal capability cannot. In addition, for claimants with low legal capability, legal advertising might overcome some of the barriers to action that exist outside compensation schemes (for example, by raising awareness about the possibility of engaging a lawyer, including on a ‘no win, no fee’ basis, and the process for doing so).[97]
Finally, socio-economically disadvantaged claimants might be more severely affected by barriers encountered during the course of their claims, as for example delays in approval of claims and provision of funds are more likely to lead to financial hardship and an urgent need for legal intervention among low, compared to high, SES claimants.[98]
The association between prior lodgement of a compensation claim and lawyer use has not been investigated in other studies of lawyer use in the Australian compensation context.[99] In the current study, prior claiming was more common among claimants who engaged lawyers than those who did not. Claimants with prior claims might struggle to apportion impairment to different injury events, leading to disputes that require legal assistance to finalise.[100] Alternatively, these claimants might have advance knowledge of the difficulties involved in navigating the compensation process and the benefits of using legal services.[101] Prior claiming has also been linked to long-term disability outcomes, perhaps due to the compounding effects of, or the complexities involved in treating, injuries from multiple events.[102]
In this study, many of the associations between the modelled variables and lawyer use appear to be the result of compensation scheme design factors (such as the degree of impairment required to claim for impairment lump sum and common law benefits, and legal cost agreements).
Claimants who entered the TAC scheme with severe injuries were more likely to use lawyers. There are several candidate explanations for this finding. First, accessing some benefits, such as impairment lump sum and common law payments, requires claimants to both have a permanent injury and undergo a potentially long and complex claiming process that can necessitate the involvement of lawyers.[103] Second, lawyers are more likely to grant access to their services when claimants have more severe injuries. This is because, in the personal injury sector in general, and in TAC claims in particular, legal services are almost exclusively provided to claimants under ‘no win, no fee’ agreements. As such, lawyers have a powerful financial incentive to select clients whose claims are likely to be successful (that is, to result in a payment of compensation) to ensure that they will be paid for their services.[104] As the success of a claim depends on the severity and permanence of claimant injuries, these factors play a crucial role in gatekeeping by lawyers in relation to their services. Third, claimants with more severe injuries may experience difficulties navigating the claiming process because of these injuries (for example, they may struggle to make decisions due to head injuries, or to concentrate due to the side effects of pain medications), leading them to seek legal assistance.[105]
The proportion of variation explained by injury severity alone was, however, much smaller than that explained by other variables. This might be because this study did not differentiate between claims based on the purposes for which lawyers were engaged. It is possible that some claimants engaged lawyers to assist with claim disputes not related to injury severity (for example, the initial acceptance of a claim, or access to a specific benefit or service). In addition, this study used an objective measure of injury severity; however, some injuries that would not be classified as serious from a clinical perspective might have a serious impact on the life of an injured person.[106] An oft-cited example is that a finger amputation might not have a high SRR or serious impact on the life of a manual labourer, but would substantially alter the life of a concert pianist.[107] This is important given that the mental and emotional impact of injuries is as dependent on subjective perceptions as on objective measures.[108]
Compensation scheme design factors might also explain some of the other associations found in the study. For example, in the TAC scheme, claimants lodging common law claims need to demonstrate that another party was negligent in their crash. Therefore, one would expect claimants other than drivers to be more likely to lodge common law claims and engage lawyers as, for example, there are few circumstances in which a passenger could be responsible for a crash. Indeed, in both cohorts, passengers and pedestrians were more likely to use lawyers than drivers. Similarly, as both impairment lump sum and common law claims depend on injury permanence, one might expect lasting injuries to be associated with both lodging these claims and using lawyers. In both cohorts, claimants with transient injuries such as ‘other injuries’ (abrasions, contusions, and lacerations) were unlikely to use lawyers, whilst those with ‘other serious injuries’ (other) (which includes amputations, degloving, loss of sight, moderate and severe burns, paraplegia, and other spinal injuries) were highly likely to use lawyers.
Understanding which claimants are most likely to engage legal services provides schemes with opportunities to intervene and minimise the risk of claimants encountering obstacles or having negative experiences that could trigger both poor recovery outcomes and lawyer use, where appropriate. Such interventions would benefit claimants through improved recovery and easier access to entitlements, and insurers through decreased costs and better performance in returning claimants to health and work. These interventions could be tailored to particular groups. For example, claimants with high legal capability could be provided with additional advice, information, and support to assist them to navigate the scheme alone; this could free up legal services for use by those with low legal capability who might struggle even with this additional support. Other examples of specific interventions could include the prompt approval of claims for low SES claimants to alleviate financial hardship; proactive case management practices (such as detailed interviews with claimants; meetings between case managers, employers, ergonomists, and occupational therapists; workplace modifications; and vocational training) to reduce work disability;[109] and early psychological interventions to prevent depression.[110]
Notably, there was little difference in the amount of variation in lawyer use explained by the models with negative recovery outcomes at three months post-crash, and the models with negative recovery outcomes as 12 months post-crash. This implies that vulnerable claimants can be identified and interventions implemented relatively soon after injury. Similarly, another study showed that experience of long-term disability and compensation-related stress can be predicted as early as three months post-injury.[111] In that study, both work disability and depression at three months post-injury were implicated in development of compensation-related stress.[112] Accordingly, interventions to combat short-term work disability, mental health, and pain issues might affect several long-term claimant outcomes relevant to subsequent lawyer engagement.
The findings of this study also have implications for access to justice, as they indicate which claimants are likely to both experience a need for legal representation and act upon that need. Notably, claimants with markers of socio-economic disadvantage, who often experience complex and severe legal problems in general (and fail to seek legal advice in response to these problems) both sought and received legal assistance in the TAC scheme. Understanding what facilitates access to justice for these disadvantaged groups in the TAC scheme could enable improved access to justice for these groups in other settings. There are, however, opportunities to improve access to justice in the TAC scheme in some groups, including among young claimants. This could be achieved by educating parents about the indemnifying role played by the TAC in their children’s claims.
This study has several limitations. First, lawyer use is likely to have been underestimated in the regressions due to the use of a limited six-year follow-up period. Second, the study used SRRs calculated using Australian hospital data; these were based only on injury survivability in hospital settings, and were not specific to Victoria.[113] In addition, SRRs were multiplied to create an overall ICISS score, a method that has been criticised as it assumes that survival probabilities are independent.[114] Third, it was not possible to control for pre-injury comorbidities or health, as this information was not available in the CRD. This was a particular issue for the non-hospitalised cohort, where the proportion of variation in lawyer use explained by the models was substantially lower than in the hospitalised cohort. This might be because, in this cohort, lawyer use might be better explained by unmeasured claimant factors. It was also an issue for the recovery indicators, as it was not possible to determine whether claimants who experienced mental health issues entered the scheme with pre-existing mental health conditions, or later developed mental health complications. Fourth, the recovery indicators were based on objective payment data rather than subjective experiences such as quality of life. Fifth, this study is restricted to compensable road traffic injury in Victoria; further research is needed to establish the factors associated with lawyer use in other compensation schemes, in Victoria and elsewhere. In addition, in jurisdictions where multiple insurers operate, it would be of value to explore whether there are differences in lawyer use between claimants whose claims are managed by different insurers.
Sixth, not all persons injured in road traffic crashes in Victoria claim compensation through the TAC scheme. Some injured persons may have minor injuries and elect to cover their medical costs themselves, or rely on their private health insurance;[115] a minority may have private income protection or disability insurance that they use instead of making a TAC claim. It is probable that choice of compensation mechanism is itself associated with legal service use (as, for example, if an injured person elects to claim through their private insurance, their legal needs might be different to an injured person who elects to claim no-fault and/or common law benefits through a compensation scheme). In addition, specific features of compensation mechanisms might be associated with legal service use (as, for example, use might be lower in schemes in which the claiming process is routinised and straightforward to navigate, and in which lawyer use is restricted; but higher in schemes in which the claiming process is complex and difficult to navigate, and in which there are institutionalised roles for lawyers). Further research is needed to determine how choice of compensation mechanism shapes the factors associated with legal service use.
Overall, despite these limitations, this study provides important empirical insight into the factors associated with lawyer use in compensation schemes. The results indicate that although injury severity and other individual-level socio-demographic, crash, and injury factors shape claimant decisions to engage lawyers, the experience of negative recovery outcomes plays by far the most important role. In the hospitalised cohort, these recovery outcomes appear to have a compounding effect, as claimants who experienced two or three negative outcomes were substantially more likely to use lawyers than those who experienced none or one. Importantly, many of the associations between the model variables and lawyer use can be attributed to compensation scheme design, suggesting that findings from one scheme are not necessarily applicable to others. There were also differences in findings across hospitalised and non-hospitalised groups in the same scheme, suggesting that not all claimant groups are homogenous in terms of their decisions to use legal services. Notably, socio-economically disadvantaged claimants, who are known to experience complex and severe problems and fail to seek legal advice in response to these problems in general, were supported to both seek and receive legal advice in the Victorian scheme. Understanding what facilitates access to justice for this group in the TAC scheme could enable improved access to justice for this group in other settings. In addition, understanding the different profiles of legal service users could inform the development of targeted interventions to assist claimants to navigate perceived system complexities and address some of the underlying reasons for lawyer use in compensation schemes.
[*] PhD Candidate, Faculty of Law, Monash University.
[**] Associate Professor, Monash University Accident Research Centre, Monash University, and Director of the Victorian Injury Surveillance Unit.
[***] Associate Professor, Monash Sustainable Development Institute and Faculty of Law, Monash University.
[****] Associate Professor, Faculty of Law, Monash University, and Director of the Australian Centre for Justice Innovation.
[1] World Health Organization, Post-Crash Response: Supporting Those Affected by Road Traffic Crashes, WHO/NMH/NVI/16.9 (2016) 3.
[2] Suzanne Polinder et al, ‘Burden of Road Traffic Injuries: Disability-Adjusted Life Years in Relation to Hospitalization and the Maximum Abbreviated Injury Scale’ (2015) 80 Accident Analysis & Prevention 193, 196–7; Juanita A Haagsma et al, ‘The Global Burden of Injury: Incidence, Mortality, Disability-Adjusted Life Years and Time Trends from the Global Burden of Disease Study 2013’ (2016) 22(1) Injury Prevention 1, 4, 7.
[3] See, eg, Peter A Cameron et al, ‘A Statewide System of Trauma Care in Victoria: Effect on Patient Survival’ (2008) 189(10) Medical Journal of Australia 546, 548; Belinda J Gabbe et al, ‘Population-Based Capture of Long-Term Functional and Quality of Life Outcomes after Major Trauma: The Experiences of the Victorian State Trauma Registry’ (2010) 69(3) The Journal of Trauma: Injury, Infection, and Critical Care 532, 532.
[4] Canadian Council of Motor Transport Administrators, Road Safety Vision 2010 (Report, November 2013) 22.
[5] S Binder and JW Runge, ‘Road Safety and Public Health: A US Perspective and the Global Challenge’ (2004) 10(2) Injury Prevention 68, 68.
[6] European Commission, Road Safety Program 2011–2020: Detailed Measures (Memo No 10/343, 20 July 2010) 3.
[7] Saber Azami-Aghdash et al, ‘Policy Analysis of Road Traffic Injury Prevention in Iran’ (2017) 9(1) Electronic Physician 3630, 3635–6. See also S Gopalakrishnan, ‘A Public Health Perspective of Road Traffic Accidents’ (2012) 1(2) Journal of Family Medicine and Primary Care 144.
[8] Richard Matzopoulos et al, ‘Assessing the Prevention Response to Child Road Traffic Injuries’ in Ashley Van Niekerk, Shahnaaz Suffla and Mohamed Seedat (eds), Crime, Violence and Injury Prevention in South Africa: Data to Action (Medical Research Council – University of South Africa Crime, Violence, and Injury Lead Program, 2008) 14, 22–3.
[9] Australian Institute of Health and Welfare, First Report on National Health Priority Areas 1996 (Report, 1997) 85–7.
[10] Ministry of Transport, ‘Safer Journeys: New Zealand’s Road Safety Strategy 2010–2020’ (Strategy Proposal, 2010) 3.
[11] World Health Organization (n 1) 4.
[12] Australian Institute of Health and Welfare, ‘ICF Australian User Guide V1.0’ (Disabilities Series No DIS 33, 10 October 2003) 93; Genevieve M Grant and David M Studdert, ‘Poisoned Chalice? A Critical Analysis of the Evidence Linking Personal Injury Compensation Processes with Adverse Health Outcomes’ [2009] MelbULawRw 29; (2009) 33(3) Melbourne University Law Review 865, 866; Peter Cane, Atiyah’s Accidents, Compensation and the Law (Cambridge University Press, 8th ed, 2013) 406–9; Genevieve M Grant, ‘Claiming Justice in Injury Law’ [2015] MonashULawRw 22; (2015) 41(3) Monash University Law Review 618, 619; Meaghan L O’Donnell et al, ‘Compensation Seeking and Disability after Injury: The Role of Compensation-Related Stress and Mental Health’ (2015) 76(8) Journal of Clinical Psychiatry e1000, e1000.
[13] Harold Luntz et al, Torts: Cases and Commentary (LexisNexis Butterworths, 8th ed, 2017) 63–6.
[14] Ibid 54–7.
[15] Darnel F Murgatroyd, Ian D Cameron and Ian A Harris, ‘Understanding the Effect of Compensation on Recovery from Severe Motor Vehicle Crash Injuries: A Qualitative Study’ (2011) 17(4) Injury Prevention 222, 224; Elizabeth Kilgour et al, ‘Interactions between Injured Workers and Insurers in Workers’ Compensation Systems: A Systematic Review of Qualitative Research Literature’ (2015) 25(1) Journal of Occupational Rehabilitation 160, 177–8; Nieke A Elbers et al, ‘Differences in Perceived Fairness and Health Outcomes in Two Injury Compensation Systems: A Comparative Study’ (2016) 16(1) BMC Public Health 658, 665 (‘Differences in Perceived Fairness and Health Outcomes’).
[16] Louis Schetzer, Joanna Mullins and Roberto Buonamano, Access to Justice & Legal Needs: A Project to Identify Legal Needs, Pathways and Barriers for Disadvantaged People in NSW (Law and Justice Foundation of NSW, 2002) 6–8; Hazel Genn, Judging Civil Justice (Cambridge University Press, 1st ed, 2010) 115.
[17] Richard Townsend Gun et al, ‘Risk Factors for Prolonged Disability after Whiplash Injury: A Prospective Study’ (2005) 30(4) Spine 386, 389; Ian A Harris et al, ‘Predictors of General Health after Major Trauma’ (2008) 64(4) The Journal of Trauma: Injury, Infection, and Critical Care 969, 970; SM Littleton et al, ‘The Association of Compensation on Longer Term Health Status for People with Musculoskeletal Injuries Following Road Traffic Crashes: Emergency Department Inception Cohort Study’ (2011) 42(9) Injury 927, 930.
[18] Gun et al (n 17) 389.
[19] J David Cassidy et al, ‘Effect of Eliminating Compensation for Pain and Suffering on the Outcome of Insurance Claims for Whiplash Injury’ (2000) 342(16) The New England Journal of Medicine 1179, 1181; J David Cassidy et al, ‘Low Back Pain after Traffic Collisions: A Population-Based Cohort Study’ (2003) 28(10) Spine 1002, 1004; Petrina P Casey, Anne Marie Feyer and Ian D Cameron, ‘Associations with Duration of Compensation Following Whiplash Sustained in a Motor Vehicle Crash’ (2015) 46(9) Injury 1848, 1851 (‘Associations with Duration of Compensation’); Bamini Gopinath et al, ‘Predictors of Time to Claim Closure Following a Non-Catastrophic Injury Sustained in a Motor Vehicle Crash: A Prospective Cohort Study’ (2016) 16(1) BMC Public Health 421, 425.
[20] Elbers et al, ‘Differences in Perceived Fairness and Health Outcomes’ (n 15) 667.
[21] Gopinath et al (n 19) 428; Casey, Feyer and Cameron, ‘Associations with Duration of Compensation’ (n 19) 1854.
[22] Kirsten Armstrong and Daniel Tess, ‘Fault versus No Fault: Reviewing the International Evidence’ (Seminar Paper, Institute of Actuaries of Australia General Insurance Seminar, 9–12 November 2008) 19–20; Harris et al (n 17) 973; Casey, Feyer and Cameron, ‘Associations with Duration of Compensation’ (n 19) 1854; Gopinath et al (n 19) 428.
[23] Cassidy et al, ‘Effect of Eliminating Compensation for Pain and Suffering on the Outcome of Insurance Claims for Whiplash Injury’ (n 19), 1184–5; Harris et al (n 17) 973; Littleton et al (n 17) 931. See also Douglas Fowlie and David Alexander, ‘Collective Actions Following Major Disaster’ (1992) 3(2) Journal of Forensic Psychiatry 321, 321–2; Paul R Lees-Haley, ‘MMPI-2 Base Rates for 492 Personal Injury Plaintiffs: Implications and Challenges for Forensic Assessment’ (1997) 53(7) Journal of Clinical Psychology 745, 752.
[24] Gun et al (n 17) 390; Natalie M Spearing et al, ‘Research on Injury Compensation and Health Outcomes: Ignoring the Problem of Reverse Causality Led to a Biased Conclusion’ (2012) 65(11) Journal of Clinical Epidemiology 1219, 1220; Petrina P Casey, Anne Marie Feyer and Ian D Cameron, ‘Associations with Legal Representation in a Compensation Setting 12 Months after Injury’ (2015) 46(5) Injury 918, 919 (‘Associations wih Legal Representation in a Compensation Setting’).
[25] Harris et al (n 17) 973; Spearing et al (n 24) 1220.
[26] Marc Galanter, ‘Reading the Landscape of Disputes: What We Know and Don’t Know (and Think We Know) about Our Allegedly Contentious and Litigious Society’ (1983) 31(1) UCLA Law Review 4, 19; Herbert M Kritzer, Risks, Reputations and Rewards: Contingency Fee Practice in the United States (Stanford University Press, 2004) 67–8 (‘Risks, Reputations and Rewards’).
[27] Grant and Studdert (n 12) 879.
[28] Australian Law Reform Commission, Managing Justice: Review of the Federal Justice System (Report No 89, 17 February 2000) 312 [5.21]; Productivity Commission, Access to Justice Arrangements: Productivity Commission Inquiry Report (Report No 72, 5 September 2014) 196.
[29] Kritzer, Risks, Reputations and Rewards (n 26) 67–8; Stephen Daniels and Joanne Martin, ‘The Texas Two-Step: Evidence on the Link between Damage Caps and Access to the Civil Justice System’ (2006) 55(2) DePaul Law Review 635, 659; Mary Nell Trautner, ‘Screening, Sorting, and Selecting in Complex Personal Injury Cases: How Lawyers Mediate Access to the Civil Justice System’ (PhD Thesis, The University of Arizona, 2006) 93–6; Grant and Studdert (n 12) 879.
[30] Herbert M Kritzer, ‘Holding Back the Floodtide: The Role of Contingent Fee Lawyers’ (1997) 70(3) Wisconsin Lawyer 10, 10–13; E Allan Lind, ‘Litigation and Claiming in Organizations: Antisocial Behavior or Quest for Justice?’ in Robert A Giacalone and Jerald Greenberg (eds), Antisocial Behavior in Organizations (Sage Publication, 1997) 150, 156; Trautner (n 29) 93–6; Jennifer K Robbenholt and Valerie P Hans, The Psychology of Tort Law (NYU Press, 2016) 13.
[31] Grant and Studdert (n 12) 879–80; Robbenholt and Hans (n 30) 13.
[32] Gun et al (n 17) 390–1.
[33] Ibid 389.
[34] Ibid 390–1.
[35] Casey, Feyer and Cameron, ‘Associations with Legal Representation in a Compensation Setting’ (n 24) 922.
[36] Ibid.
[37] Ibid; Gun et al (n 17) 389–91.
[38] Casey, Feyer and Cameron, ‘Associations with Legal Representation in a Compensation Setting’ (n 24) 920–2; Darnel Murgatroyd et al, ‘Predictors of Seeking Financial Compensation Following Motor Vehicle Trauma: Inception Cohort with Moderate to Severe Musculoskeletal Injuries’ (2017) 18(1) BMC Musculoskeletal Disorders 177, 183–4.
[39] Casey, Feyer and Cameron, ‘Associations with Legal Representation in a Compensation Setting’ (n 24).
[40] Murgatroyd et al (n 38) 178.
[41] Nick Allsop, Hardik Dalal and Peter McCarthy, ‘To Fault or Not to Fault That Is the Question?’ (Seminar Paper, Institute of Actuaries of Australia Accident Compensation Seminar, 22–24 November 2009) 5; Cassidy et al, ‘Effect of Eliminating Compensation for Pain and Suffering on the Outcome of Insurance Claims for Whiplash Injury’ (n 19) 1181.
[42] Grant and Studdert (n 12) 877–8.
[43] Compensation is also available to persons injured interstate if the crash involved a Victorian-registered vehicle, and to dependents of a person killed in a transport crash if the decedent would have been entitled to compensation: Transport Accident Act 1986 (Vic) s 35.
[44] In order to access these benefits, claimants need to contact the TAC or file a claims form within 12 months of the crash date: Transport Accident Act 1986 (Vic) s 68(1).
[45] Transport Accident Act 1986 (Vic) s 47(1)–(3).
[47] Ibid s 46A(1A).
[48] Transport Accident Commission, ‘Transport Accident Act Common Law Protocols’ (Protocol, 1 July 2016) <http://www.tac.vic.gov.au/__data/assets/pdf_file/0004/181390/FINAL-Common-Law-Protocols-as-at-22.12.2015.pdf> [16].
[49] Transport Accident Commission, ‘Transport Accident Act No Fault Dispute Resolution Protocols’ (Protocol, 1 July 2016) <http://www.tac.vic.gov.au/__data/assets/pdf_file/0004/181399/No-Fault-Dispute-Resolution-Protocols-July-2016.pdf> .
[50] In 2005, the TAC, the Law Institute of Victoria, and the Australian Lawyers Alliance published a series of Protocols that seek to (a) recognise the role played by lawyers in the TAC scheme, and (b) provide guidelines to govern the ways in which lawyers and insurers interact to deliver outcomes to claimants. The Protocols are designed to facilitate the mutual and early exchange of relevant information between lawyers and the TAC, minimise delays by enforcing compliance with specified timeframes, fix legal costs for routine activities, reduce adversarialism in the claiming process, and encourage the early resolution of disputes. In doing so, the Protocols set the duration of activities in legal claims (affecting the duration of legal service use) and the amount that can be paid to lawyers (affecting the cost of legal service use) for firms that voluntarily become signatories to these protocols: Transport Accident Commission, ‘Transport Accident Act No Fault Dispute Resolution Protocols’ (n 49); Grant and Studdert (n 12) 883–4.
[51] Transport Accident Commission, ‘Legal Costs Recovery Guidelines’ (Guidelines, 10 November 2016) 14. See also Supreme Court (General Civil Procedure) Rules 2015 (Vic) ord 26.
[52] Legal Profession Uniform Law Application Act 2014 (Vic) sch 1 s 182.
[54] Institutional ethics approval for this study was obtained from the Monash University Human Research Ethics Committee (Project Number: 11752).
[55] Khic-Houy Prang, Behrooz Hassani-Mahmooei and Alex Collie, ‘Compensation Research Database: Population-Based Injury Data for Surveillance, Linkage and Mining’ (2016) 9(1) BMC Research Notes 456, 458. For a full list of the variables contained in the CRD see generally, Institute for Safety Compensation and Recovery Research, ‘TAC Data Dictionary’ (Data Dictionary No 8.2, August 2014) <https://research.iscrr.com.au/__data/assets/pdf_file/0003/297930/tac_data_dictionary_version_82.pdf>.
[56] Interstate claims were excluded because entitlement to common law damages is determined in accordance with the law of the state or territory in which a crash occurs, rather than Victorian law.
[57] Claims for fatalities were excluded because these relate to the needs of surviving dependents, which are manifestly different to the needs of injured persons.
[58] Of the removed claims, 14.9% related to multiple claims arising from a single incident, and 85.1% to multiple claims arising from multiple incidents.
[59] This is comparable to the 70.9% of individuals that live in major cities in Australia as a whole. Transport and Regional Economics Bureau of Infrastructure, ‘An Introduction to Where Australians Live’ (Information Sheet No 96, 2016) 8.
[60] Based on the CRD payments data used in the analyses (see Part II(B): Variables Used in Analyses).
[61] Clare E Scollay, Janneke Berecki-Gisolf and Genevieve Grant, Trends in Lawyer Use in Road Traffic Injury Compensation Claims (Unpublished Manuscript, Monash University, 2019).
[62] Transport Accident Act 1986 (Vic) s 46A(1A).
[63] Scollay, Berecki-Gisolf and Grant (n 61).
[64] Australian Bureau of Statistics, Remoteness Structure (15 March 2018) <http://www.abs.gov.au/websit edbs/D3310114.nsf/home/remoteness+structure> .
[65] See generally Australian Bureau of Statistics, An Introduction to Socio-Economic Indexes for Areas (SEIFA): Technical Paper (Catalogue No 2039.0.55.001, 2006).
[66] Shaun Stephenson et al, Australian Institute of Health and Welfare, Diagnosis-Based Injury Severity Scaling: A Method Using Australian and New Zealand Hospital Data Coded to ICD-10-AM (Injury Research and Statistics Series, 2003) 24–73.
[67] For an overview of methodologies for combining SRRs: Geoff Henley and James E Harrison, Injury Severity Scaling: A Comparison of Methods for Measurement of Injury Severity (Injury Research and Statistics Series No 10, June 2009) 3.
[68] Pharmaceutical Benefits Scheme (PBS) (Web Page) <http://www.pbs.gov.au/pbs/home> .
[69] ‘ATC/DDD Index 2018’, World Health Organization Collaborating Centre for Drug Statistics Methodology (Web Page, 13 December 2018) <https://www.whocc.no/atc_ddd_index/>.
[70] For prior use of this method, see Janneke Berecki-Gisolf et al, ‘Use of Antidepressant Medication after Road Traffic Injury’ (2015) 46(7) Injury 1250, 1251; Janneke Berecki-Gisolf et al, ‘Prescription Opioid and Benzodiazepine Use after Road Traffic Injury’ (2016) 17(2) Pain Medicine 304, 306.
[71] Data were analysed using SAS 9.4 for Windows and SPSS Statistics 23.0.
[72] See generally John W Tukey, ‘One Degree of Freedom for Non-Additivity’ (1949) 5(3) Biometrics 232.
[73] See generally Hirotogu Akaike, ‘Information Theory and an Extension of the Maximum Likelihood Principle’ in Emanuel Parzen, Kunio Tanabe and Genshiro Kitagawa (eds), Selected Papers of Hirotugu Akaike (Springer, 1998) 199.
[74] See generally Tue Tjur, ‘Coefficients of Determination in Logistic Regression Models – A New Proposal: The Coefficient of Discrimination’ (2009) 63(4) The American Statistician 366.
[75] Interaction effects between the recovery outcomes and other variables were explored but did not improve the fit of the model (ie, the Link Test remained significant in the models with the interaction effects added), suggesting that there may be a variable missing from the model. At fault status (according to police report) was investigated as a possible missing variable for the N=13,508 (82.8%) claimants who had this data available. Although at fault status was significantly associated with lawyer use, the Link Test remained significant, suggesting that this is not the variable missing from the model. As the data were limited to the variables contained in the CRD, no further alternatives could be explored. The AIC suggested that the model with the recovery outcomes was the best fitting model.
[77] In these studies, legal problems are defined as problems for which the law provides a potential avenue for resolution, regardless of whether or not legal action is ultimately taken. The legal problems examined differ across studies, but tend to include consumer, community, employment, family, finance, housing, public bureaucracy, and economic and personal injury legal problems: Hazel Genn, Paths to Justice: What People Do and Think about Going to Law (Hart Publishing, 1999) 12; Rebecca L Sandefur, ‘Access to Civil Justice and Race, Class, and Gender Inequality’ (2008) 34 Annual Review of Sociology 339, 343; Ab Currie, ‘The Legal Problems of Everyday Life’ (2009) 12 Sociology of Crime, Law, and Deviance 1, 8.
[78] Christine Coumarelos et al, Law and Justice Foundation of New South Wales, Legal Australia-Wide Survey: Legal Need in Australia (Access to Justice and Legal Needs No 7, August 2012) 104.
[79] Ibid 69–70.
[80] Ibid 146. Note that in the Legal Australia-Wide Survey, respondents were asked whether their legal problem was ongoing or over; problems were categorised as finalised if the respondent stated that the problem was over. Problems could be categorised as finalised even if the respondent had decided not to take any steps to resolve the problem.
[81] Transport Accident Act 1986 (Vic) s 46A(1)(b).
[82] Limitation of Actions Act 1958 (Vic) s 27E.
[83] Australian Law Reform Commission, Seen and Heard: Priority for Children in the Legal Process (Report No 84, 19 November 1997) 51.
[84] Ibid 51–2.
[85] Casey, Feyer and Cameron, ‘Associations with Legal Representation in a Compensation Setting’ (n 24) 920–2.
[86] Fowlie and Alexander (n 23) 326; Katherine Lippel, ‘Therapeutic and Anti-Therapeutic Consequences of Workers’ Compensation’ (1999) 22(5– 6) International Journal of Law and Psychiatry 521, 524–5; Grant, ‘Claiming Justice in Injury Law’ (n 12) 641; Kilgour et al (n 15) 178.
[87] Fowlie and Alexander (n 23) 322–3; Valerie Tarasuk and Joan M Eakin, ‘The Problem of Legitimacy in the Experience of Work-Related Back Injury’ (1995) 5(2) Qualitative Health Research 204, 208–10; Lippel (n 86) 533–4; Lee Strunin and Leslie I Boden, ‘The Workers’ Compensation System: Worker Friend or Foe?’ (2004) 45(4) American Journal of Industrial Medicine 338, 341–2; David A Alexander, Raj Badial and Susan Klein, ‘Personal Injury Compensation: No Claim without Pain?’ (2006) 30(10) Psychiatric Bulletin 373, 374; Murgatroyd, Cameron and Harris (n 15) 225; Kilgour et al (n 15) 164–9.
[88] Steven R Smith, ‘Malpractice Liability of Mental Health Professionals and Institutions’ in Bruce D Sales and Daniel W Shuman (eds), Law, Mental Health, and Mental Disorder (Brooks/Cole Publishing Company, 1996) 76, 85; Daniel W Shuman, ‘When Time Does Not Heal: Understanding the Importance of Avoiding Unnecessary Delay in the Resolution of Tort Cases’ (2000) 6(4) Psychology, Public Policy, and Law 880, 887.
[89] Marc Galanter, ‘Predators and Parasites: Lawyer-Bashing and Civil Justice’ (1994) 28(3) Georgia Law Review 633, 634–6.
[90] Gun et al (n 17); Darnel F Murgatroyd et al, ‘Predictors of Return to Work Following Motor Vehicle Related Orthopaedic Trauma’ (2016) 17(1) BMC Musculoskeletal Disorders 171, 176.
[91] Coumarelos et al (n 78) 104.
[92] Ibid 146.
[93] Community Law Australia, Unaffordable and Out of Reach: The Problem of Access to the Australian Legal System (Report, July 2012) 6.
[94] Ibid 6–7, 9–10; Amanda Alford and James Farrell, ‘Community Legal Centres Face Funding Crisis’ (2016) 41(1) Alternative Law Journal 2, 2.
[95] Coumarelos et al (n 78) 29–31; Hugh M McDonald and Julie People, ‘Legal Capability and Inaction for Legal Problems: Knowledge, Stress and Cost’ (2014) 41 Updating Justice 1, 2; Pascoe Pleasence et al, ‘Reshaping Legal Assistance Services: Building on the Evidence Base’ (Discussion Paper, Law and Justice Foundation of New South Wales, April 2014) 130–1.
[96] Coumarelos et al (n 78) 36–7; Pascoe Pleasence and Nigel J Balmer, How People Resolve ‘Legal’ Problems: A Report to the Legal Services Board (Report, May 2014) 100–1.
[97] Albert J Hudec and Michael J Trebilcock, ‘Lawyer Advertising and the Supply of Information in the Market for Legal Services’ (1982) 20(1) University of Western Ontario Law Review 53, 54; Nora Freeman Engstrom, ‘Sunlight and Settlement Mills’ (2011) 86(4) New York University Law Review 805, 853; Richard Lewis and Annette Morris, ‘Tort Law Culture: Image and Reality’ (2012) 39(4) Journal of Law and Society 562, 586.
[98] For evidence of delays and their effects, see, eg, Bridget Bryant, Richard Mayou and Sally Lloyd-Bostock, ‘Compensation Claims Following Road Accidents: A Six-Year Follow-Up Study’ (1997) 37(4) Medicine, Science and the Law 326, 326; Nieke A Elbers et al, ‘Do Compensation Processes Impair Mental Health? A Meta-Analysis’ (2013) 44(5) Injury 674, 681; Belinda J Gabbe et al, ‘Financial and Employment Impacts of Serious Injury: A Qualitative Study’ (2014) 45(9) Injury 1445, 1450; Elbers et al, ‘Differences in Perceived Fairness and Health Outcomes’ (n 15) 668.
[99] However, one study did compare the proportion of claimants who used a lawyer and had a prior claim to the proportion of claimants who did not use a lawyer and had a prior claim: Casey, Feyer and Cameron, ‘Associations with Legal Representation in a Compensation Setting’ (n 24) 920–2.
[100] Casey, Feyer and Cameron, ‘Associations with Legal Representation in a Compensation Setting’ (n 24) 923.
[101] Marc Galanter, ‘Why the “Haves” Come Out Ahead: Speculations on the Limits of Legal Change’ (1974) 9(1) Law & Society Review 95, 97–101.
[102] Casey, Feyer and Cameron, ‘Associations with Legal Representation in a Compensation Setting’ (n 24) 923.
[103] Murgatroyd, Cameron and Harris (n 15). See also Elbers et al, ‘Differences in Perceived Fairness and Health Outcomes’ (n 15).
[104] Grant and Studdert (n 12) 879.
[105] Genevieve Grant, The Claims, Advice and Decisions after Injury (CADI) Study: Interviews with Claimants (Final Report, Monash University, May 2017) 53.
[106] Deborah R Hensler et al, Compensation for Accidental Injuries in the United States (Report, 1991) 44.
[107] Tony Buzzard, ‘Transport Accident Compensation: A Medical Point of View’ in David Miles (ed) Motor Car Injuries: Transport Accident Act (Leo Cusson Institute, 1987) cited in Ian Malkin, ‘Victoria’s Transport Accident Reforms: In Perspective’ [1987] MelbULawRw 19; (1987) 16(2) Melbourne University Law Review 254, 271.
[108] Hensler et al (n 106) 44.
[109] See, eg, Bengt B Arnetz et al, ‘Early Workplace Intervention for Employees with Musculoskeletal-Related Absenteeism: A Prospective Controlled Intervention Study’ (2003) 45(5) Journal of Occupational and Environmental Medicine 499, 501–2.
[110] See, eg, Charles F Reynolds III et al, ‘Early Intervention to Reduce the Global Health and Economic Burden of Major Depression in Older Adults’ (2012) 33(1) Annual Review of Public Health 123, 126–8.
[111] Matthew J Spittal et al, ‘Development of Prediction Models of Stress and Long-Term Disability among Claimants to Injury Compensation Systems: A Cohort Study’ (2018) 8(4) BMJ Open 1, 7.
[112] Ibid 4.
[113] Stephenson et al (n 66) 20.
[114] Ibid.
[115] Grant and Studdert (n 12) 877; Linda J Carroll et al, ‘Complexities in Understanding the Role of Compensation-Related Factors on Recovery from Whiplash-Associated Disorders: Discussion Paper 2’ (2011) 36(25S) Spine S316, S317. Some claimants also elect to claim medical benefits through a private insurer and then later lodge a TAC claim. In these cases, once the TAC claim has been accepted, the TAC can reimburse the private insurer: ‘Private Health Insurance: Reimbursement of Expenses’, Transport Accident Commission (Policy) <http://www.tac.vic.gov.au/clients/what-we-can-pay-for/policies/other /private-health-insurance-reimbursement-of-expenses#targetText=Treatment%20and %20services %20resulting%20from,the%20fund%20for%20these%20services> .
AustLII:
Copyright Policy
|
Disclaimers
|
Privacy Policy
|
Feedback
URL: http://www.austlii.edu.au/au/journals/UNSWLawJl/2020/4.html